What Is the Discharge Summary and Why Is It Important?

by Vince Hartman
Nov 28, 2022
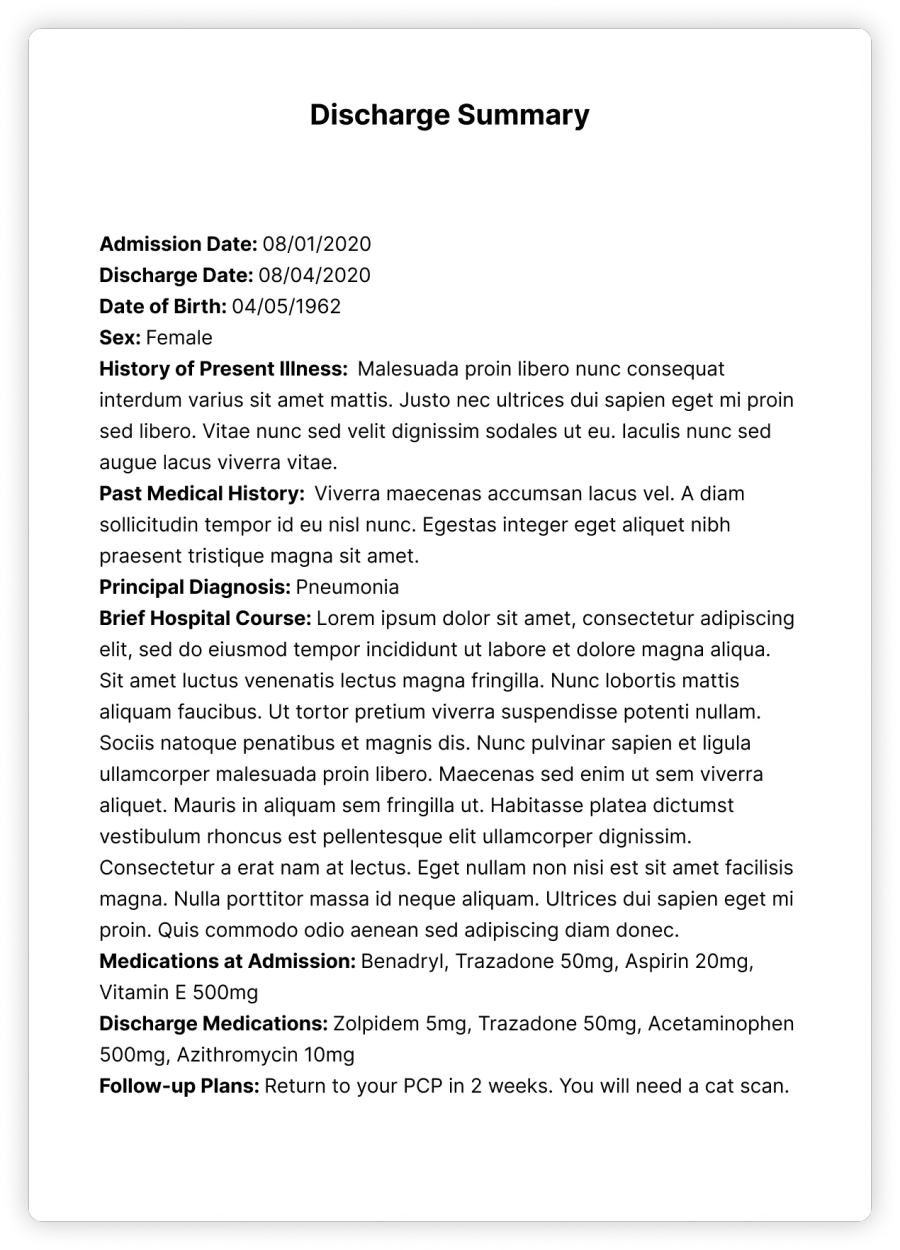
The discharge summary is a narrative document for communicating clinical information about what happened to the patient in the hospital. It’s extremely important for telling primary care doctors and other outpatient providers which follow-ups are needed for the patient.
It is really challenging nowadays in healthcare to quickly understand a patient’s medical record. In other domains outside of healthcare — such as law, news, movies, and literature — you can read a summarized version of the content to understand the main points. In healthcare, the closest synopsis is the Discharge Summary: it serves to inform all other clinicians what has happened to the patient while in the hospital and what sort of continuing care the patient requires, which is arguably why it is the most important document a hospitalist writes. Keep in mind though, this document is only for summarizing the hospital patient stay; there does not exist a narrative summary of the complete medical record. Hospitalists nowadays have little time to write a good Discharge Summary; the quality definitely varies among physicians. And oftentimes the Discharge Summary can be delayed to downstream outpatient physicians (primary care providers), causing a disruption in the continuity of care and risking patient readmissions and poor health outcomes. None of this is intentional; if a patient has been in-house for months with different hospitalists, different medical units, and different treatments, crafting a good summary is challenging.
The Discharge Summary is regulated by the Joint Commission (JCAHO) which is responsible for accreditation of healthcare organizations — i.e if a hospital has poorly written Discharge Summaries, they receive an audit from JCAHO. Thus, the Discharge Summary has pretty clear mandatory elements: what was the patient’s history, why were they hospitalized, what were the significant events during their stay including procedures and treatments, in what condition did the patient leave the hospital, and what sort of follow-ups are required after discharge including medications. Like any good story, the quality goes into how well these required elements are all weaved together.
So, what makes a good Discharge Summary?
In our conversations with physicians that we interviewed, it is definitely a learned skill that is acquired overtime through medical school and residency training. The doctor needs to balance the correct amount of conciseness without leaving out content that would be considered medically necessary. Our interviewees commonly stated that med students tend to write summaries that are closer to novels and are just way too long; medical conciseness is an artform.
Procrastination though affects everyone including doctors; and manually writing these summaries soon feels like a repetitively rote task — similar to logging one’s hours at work every week. The best policy practices we’ve seen for ensuring a good Discharge Summary is for the hospital to instruct doctors to strategically update it each day during a patient’s stay and not procrastinate it till discharge. These hospitals have a running hospital course section where doctors write a few sentences each day of the previous patient interval history. And then by discharge, this running patient course is stitched together to become the hospital course section of the Discharge Summary. And then the majority of the other elements of the Discharge Summary (with the exception of medication reconciliation) are auto-populated through a note template. While a discharge summary can take 30 minutes to 2 hours to write on average if one waits till discharge, the process is slightly faster through a daily approach. It’s like documenting your hours for the week — it’s a lot easier to document what you did each day than waiting till the end of the week to think back about what happened. The challenge with the approach though is that one individual is not consistently writing this compiled summary — it’s the responsibility of each physician to write their interval for the patient during their rounds. So by discharge, the summary will have different styles narratively. Secondly, if one physician procrastinates to write a narrative during the stay, it throws off the whole system. And more concerning, the discharging physician has no tools to confirm the validity of what was written — you are just accepting as a matter of fact the narrative. For this reason and others, outpatient general practitioners commonly find mistakes in the Discharge Summary. This stitched together narrative approach is the best of what has been available to date.
Automating the Discharge Summary
With Abstractive Health, we’ve taken the best of the daily narrative approach during the patient stay and automated it for review for the physician at any given point. Our software can extract all of the salient information from the physician progress notes, procedure notes, labs, and other data and craft that interval sentences so the physician doesn’t need to take the time to do that every day. The best part is that we can link our summary sentences back to the original source notes, so physicians can understand what is driving the content behind our automation.
By automating the Discharge Summary, we’ve taken the first steps of building that patient synopsis for healthcare. Doctors are trained in medical school through these narrative stories, which is exactly why the Discharge Summary is so important. And humans in general are cognitively designed to understand a good story better than just facts. That is why we are solving the burnout and big data problem in healthcare through a narrative summary — the story of each patient behind the data.
Abstractive Health provides an automated narrative summary of the medical record as a software solution for healthcare. We use a natural language processing algorithm to summarize the most important and salient information in the patient chart. We currently have a partnership with Weill Cornell where we are demonstrating the clinical quality of our automated hospital summaries compared to the hospital course section of the Discharge Summary.

See the Abstractive Health AI assistant in action to discover what real efficiency can look like.
Try for freeStay ahead of the curve in healthcare innovation.
Connect
Abstractive Health
Resources
©2026 Abstractive Health. All Rights Reserved.
